Haemorrhoids are collections of submucosal, fibrovasular, arteriovenous sinusoids that are part of the normalanorectum1
Symptoms include painless rectal bleeding during defaecation with or without prolapse (most common), anal pruritis or pain, and a lump at the anal verge from thrombosis or strangulation1
Most patients with low-grade internal haemorrhoids will experience relief with home-based conservative treatment or office-based procedures1
Surgery is indicated for low-grade haemorrhoids that are refractory to conservative treatment, high-grade haemorrhoids and complicated haemorrhoids1
Classification of haemorrhoids
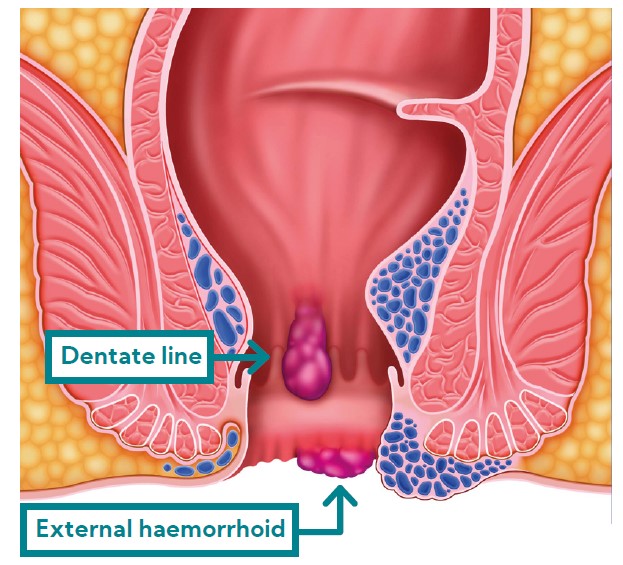
Haemorrhoids can be internal, external or mixed, depending on their relationship to the dentate line1
Internal haemorrhoids originate from above the dentate line and are less sensitive to pain due to visceral innervation-amenable to office-based procedures with minimal or no anaesthesia1
External haemorrhoids originate from below the dentate line and are sensitive to pain due to somatic innervation– anaesthesia is necessary if treatedsurgically1
Mixed internal and external haemorrhoids straddle the dentate line and are treatedas external haemorrhoids1
Internal haemorrhoids are further subclassified into 4 grades depending on the degree of prolapse:1
Conservative treatment for all patients
Most patients with new-onset symptomatic haemorrhoids can be treated conservatively for as long as needed with dietary/lifestyle modification, and topical or oral medications to relieve symptoms1
Dietary and lifestyle modification
Increased fibre intake improves symptoms of bleeding, mild prolapse, irritation and pruritis1
Patients should ingest 20-30 g of insoluble fibre per day either through diet or supplements, and increase water intake to 1.5 to 2 litres a day1
Patients should be advised to refrain from straining or lingering on the toilet, to exercise, avoid medications that cause constipation or diarrhoea and to limit their intake of fatty foods and alcohol1
Medications for symptomatic relief
Hydrocortisone-lidocaine combinations are effective for relieving acute pain and topical steroids may relieve associated pruritis and shrink the haemorrhoids1
Venoactive agents or phlebotonics improve venous tone and may reduce bleeding, as well as other symptoms such as pruritis1
Warm sitz baths 2-3 times a day reduce inflammation and oedema and relax anal sphincter tone1
Reasons to refer to a specialist
Symptomatic low-grade (I or II) internal haemorrhoids refractory to 6-8 weeks of medical treatment.1
Symptomatic high-grade (III or IV) internal haemorrhoids.1
Thrombosed haemorrhoids, with the exception of subacute (older than three days) thrombosed external haemorrhoids, which can be managed expectantly with resolution of symptoms expected in 7 to 10 days.1
Patients ≥ 40 years old with rectal bleeding should be referred for colonoscopy.1
Patients with haemorrhoids and one of the following conditions should be referred for colonoscopyregardless of age: anaemia, bleeding, concomitant change in bowel patterns, personal history of colorectalpolyps, family history of inflammatory bowel disease or colorectal cancer in a first-degree relative, or othersuspected pathologic pelvic changes that could contribute to the patient’s symptoms.1
Office-based procedures for symptomatic haemorrhoids
Recommended for patients with symptomatic grade I, II, or III internal haemorrhoids refractory to conservativetreatment.1
Common procedures include rubber band ligation, sclerotherapy, infrared coagulation of internal haemorrhoids, and excision of thrombosed external haemorrhoids.1
Rubber band ligation is preferred for healthy patients with grade I, II, or III internal haemorrhoids, whereas sclerotherapy is preferred for patients who are on anticoagulants, are immunocompromised or have portalhypertension.1
Acutely thrombosed external haemorrhoids can be excised if patient presents within the first 3 days of symptoms.1
Grade IV internal haemorrhoids require definitive surgical treatment.1
References
Reference: 1. Bleday R, Breen E. UpToDate 2022; [cited 10 March 2022]; Available from: www.uptodate.com.
Under licence from Karo Pharma Stockholm, Sweden. For full prescribing information refer to the professional information approved by the medicines regulatory authority.
Adcock Ingram Limited. Co. Reg. No. 1949/034385/06. Private Bag X69, Bryanston, 2021, South Africa. Customer Care: 0860 ADCOCK/232625. www.adcock.com. 2022033110193661. March 2022.